
Retinoids: Everything You Need to Know About These Powerful Skin Treatments
Introduction
Among all therapeutic agents used in dermatology, retinoids remain one of the most extensively researched and clinically valuable classes of compounds. Derived from vitamin A, retinoids have transformed the management of numerous skin disorders, particularly acne vulgaris, photoaging, hyperpigmentation, psoriasis, and disorders of keratinization. Their unique ability to regulate cellular growth, differentiation, inflammation, and collagen synthesis has established them as the cornerstone of modern dermatologic therapy.
Over the past five decades, retinoid science has evolved from the discovery of vitamin A deficiency-related skin abnormalities to the development of highly selective synthetic retinoids targeting specific receptors. Today, dermatologists utilize both topical and systemic retinoids to treat a wide spectrum of skin diseases, while cosmetic formulations containing retinol and retinaldehyde dominate the anti-aging skincare market.
This article provides a detailed understanding of retinoids, their relationship with vitamin A metabolism, historical development, therapeutic evolution, and their critical role in contemporary dermatology.
What Are Retinoids?
Definition of Retinoids
Retinoids are a group of natural and synthetic compounds structurally and functionally related to vitamin A (retinol). They exert their biological effects by interacting with specific nuclear receptors that regulate gene expression involved in cell proliferation, differentiation, apoptosis, and immune responses. In simple terms, retinoids are substances that help skin cells grow, mature, and function normally.
Key Characteristics of Retinoids
Retinoids:
- Are derivatives of vitamin A
- Influence cellular differentiation
- Regulate keratinization
- Stimulate collagen production
- Reduce inflammation
- Accelerate epidermal turnover
- Improve skin texture and pigmentation
These properties explain why retinoids are considered the gold standard treatment for acne and photoaging.
Classification of Retinoids
Retinoids are generally categorized into natural and synthetic forms.
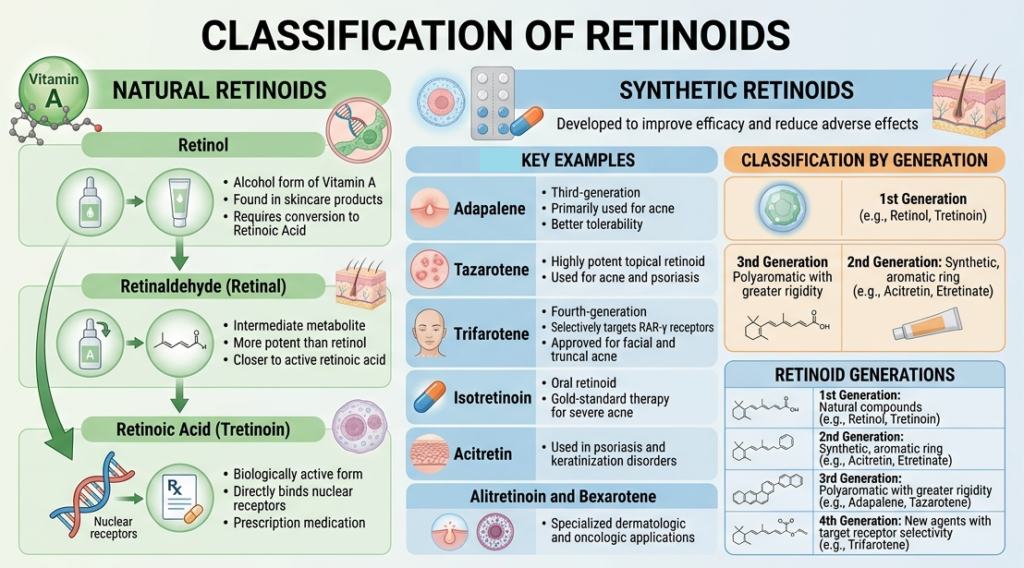
Natural Retinoids
Natural retinoids are directly involved in vitamin A metabolism.
Retinol
- Alcohol form of vitamin A
- Found in skincare products
- Requires conversion to retinoic acid
Retinaldehyde (Retinal)
- Intermediate metabolite
- More potent than retinol
- Closer to active retinoic acid
Retinoic Acid (Tretinoin)
- Biologically active form
- Directly binds nuclear receptors
- Prescription medication
Synthetic Retinoids
Synthetic retinoids were developed to improve efficacy and reduce adverse effects.
Examples include:
Adapalene
- Third-generation retinoid
- Primarily used for acne
- Better tolerability
Tazarotene
- Highly potent topical retinoid
- Used for acne and psoriasis
Trifarotene
- Fourth-generation retinoid
- Selectively targets RAR-γ receptors
- Approved for facial and truncal acne
Isotretinoin
- Oral retinoid
- Gold-standard therapy for severe acne
Acitretin
- Used in psoriasis and keratinization disorders
Alitretinoin and Bexarotene
- Specialized dermatologic and oncologic applications
Retinoids are commonly classified into four generations based on their molecular structure and receptor selectivity.
Understanding Endogenous Vitamin A Metabolism
To understand retinoids, it is essential to understand how vitamin A is metabolized within the human body.
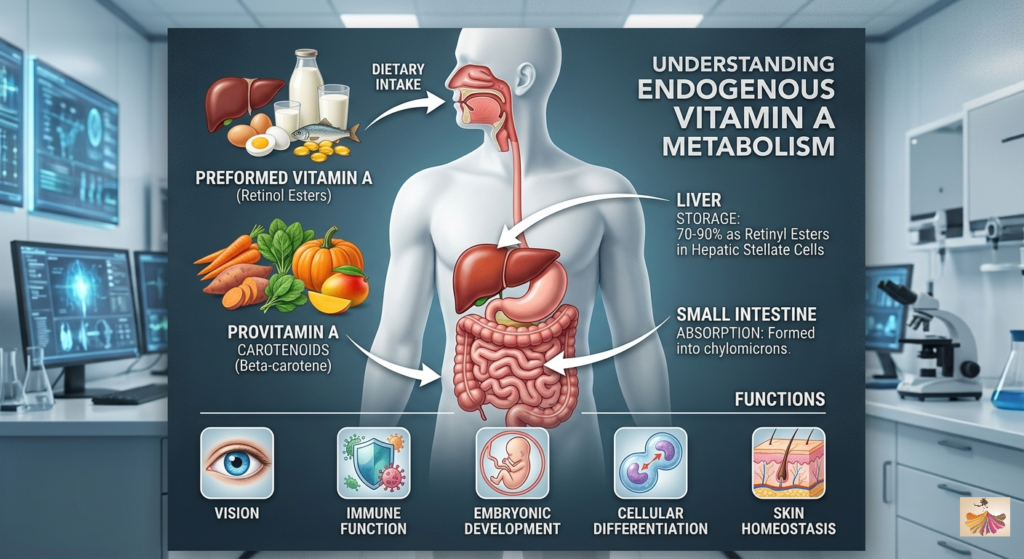
What Is Vitamin A?
Vitamin A is a fat-soluble vitamin essential for:
- Vision
- Immune function
- Embryonic development
- Cellular differentiation
- Skin homeostasis
Vitamin A exists in two major dietary forms:
Preformed Vitamin A
Found in:
- Liver
- Eggs
- Dairy products
- Fish oils
Mainly present as retinol esters.
Provitamin a Carotenoids
Found in:
- Carrots
- Sweet potatoes
- Spinach
- Pumpkin
- Mangoes
The most important carotenoid is beta-carotene.
Absorption and Storage
After ingestion:
- Vitamin A is absorbed in the small intestine.
- It is incorporated into chylomicrons.
- Transported to the liver.
- Stored as retinyl esters in hepatic stellate cells.
Approximately 70–90% of body vitamin A reserves are stored in the liver.
Conversion Pathway of Vitamin A
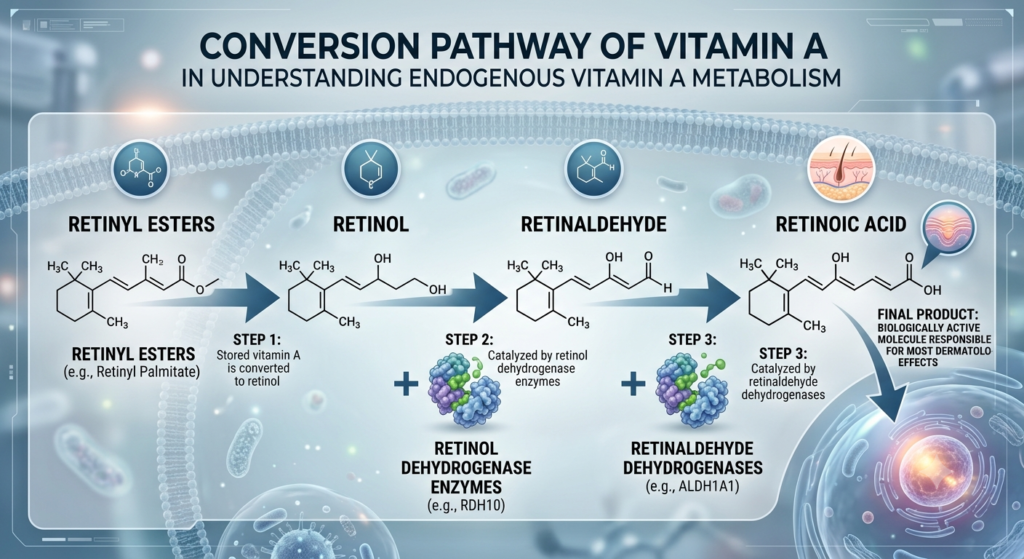
The metabolic pathway follows:
Step 1: Retinyl Esters → Retinol
Stored vitamin A is converted to retinol.
Step 2: Retinol → Retinaldehyde
Catalyzed by retinol dehydrogenase enzymes.
Step 3: Retinaldehyde → Retinoic Acid
Catalyzed by retinaldehyde dehydrogenases.
This final product is retinoic acid which is the biologically active molecule responsible for most dermatologic effects.
Mechanism of Action in Skin Cells
Retinoic acid enters skin cells and binds to:
Retinoic Acid Receptors (RARs)
- RAR-α
- RAR-β
- RAR-γ
Retinoid X Receptors (RXRs)
- RXR-α
- RXR-β
- RXR-γ
These receptors regulate the transcription of hundreds of genes involved in:
- Epidermal differentiation
- Sebaceous gland activity
- Inflammation
- Collagen synthesis
- Melanogenesis
This gene-regulating ability makes retinoids exceptionally powerful therapeutic agents.
Historical Discovery of Retinoids in Dermatology
Early Recognition of Vitamin A Deficiency

The story of retinoids began in the early 20th century when scientists observed that vitamin A deficiency caused:
- Xerosis (dry skin)
- Follicular hyperkeratosis
- Visual disturbances
Researchers recognized that vitamin A played an essential role in maintaining epithelial tissues.
Discovery of Vitamin A
Vitamin A was first identified in 1913 by independent research groups investigating nutritional deficiencies. Over subsequent decades, scientists discovered that vitamin A was vital for normal epithelial differentiation.
Discovery of Retinoic Acid
During the mid-20th century, researchers isolated and characterized retinoic acid as the biologically active metabolite of vitamin A. This discovery revolutionized dermatologic research because retinoic acid could directly influence skin cell behavior.
Introduction of Tretinoin
One of the most important milestones occurred in the late 1960s and early 1970s.
Researchers discovered that:
- Tretinoin normalized follicular keratinization
- Reduced comedone formation
- Improved acne lesions
In 1971, topical tretinoin became one of the first FDA-approved retinoid treatments for acne. This marked the beginning of modern retinoid therapy.
Evolution of Retinoid-Based Dermatologic Therapy
The development of retinoids can be divided into several phases.
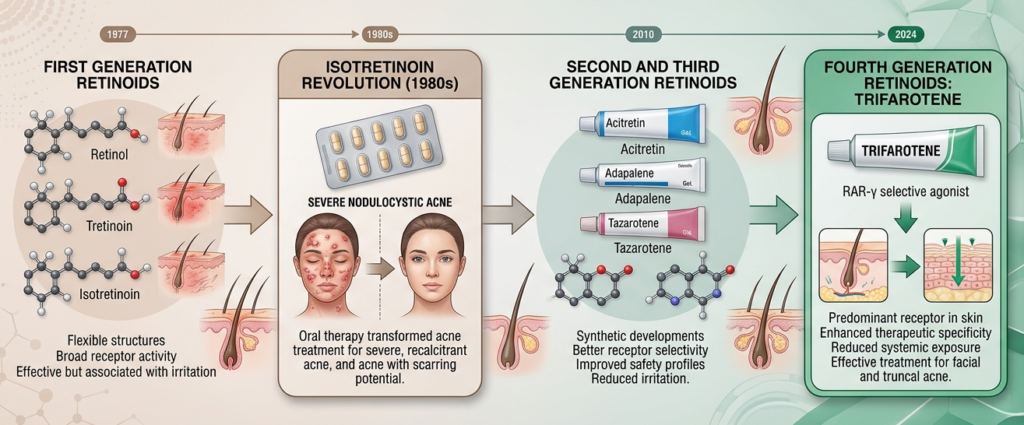
First Generation Retinoids
Examples:
- Retinol
- Tretinoin
- Isotretinoin
Characteristics:
- Flexible molecular structures
- Broad receptor activity
- Effective but associated with irritation
Isotretinoin Revolution
The introduction of oral isotretinoin in the 1980s transformed acne treatment.
For the first time, dermatologists could effectively treat:
- Severe nodulocystic acne
- Recalcitrant acne
- Acne with scarring potential
Isotretinoin remains the most effective long-term treatment for severe acne.
Second and Third Generation Retinoids
Scientists developed synthetic retinoids with:
- Better receptor selectivity
- Improved safety profiles
- Reduced irritation
Examples include:
- Acitretin
- Adapalene
- Tazarotene
Fourth Generation Retinoids
The newest advancement is trifarotene, a selective RAR-γ agonist.
RAR-γ is the predominant retinoid receptor in the skin.
Benefits include:
- Enhanced therapeutic specificity
- Reduced systemic exposure
- Effective treatment of facial and truncal acne
Trifarotene represents the first new retinoid molecule approved in over two decades.
Mechanisms That Make Retinoids Effective
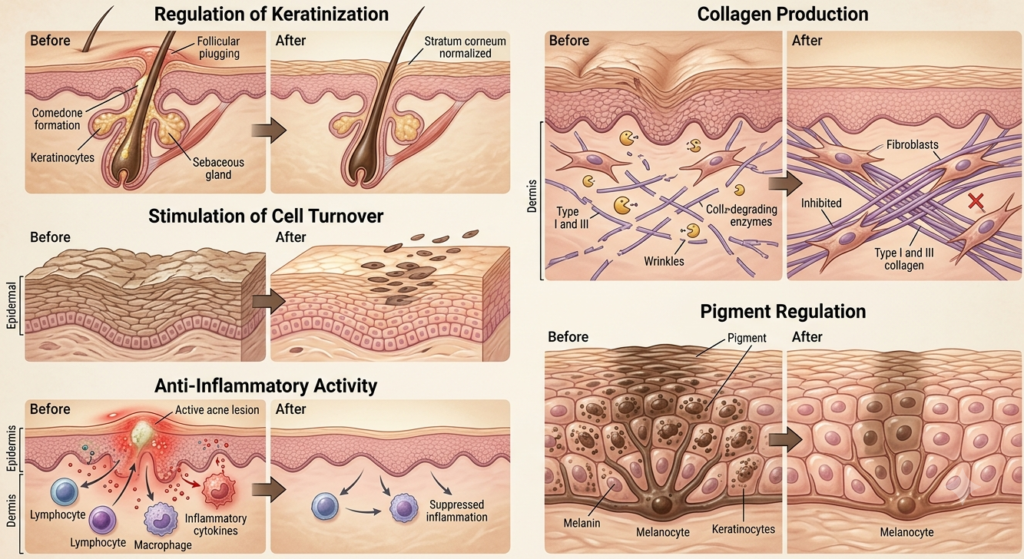
Regulation of Keratinization
Retinoids normalize epidermal differentiation.
This prevents:
- Follicular plugging
- Comedone formation
- Hyperkeratosis
Stimulation of Cell Turnover
Retinoids increase epidermal renewal.
Benefits include:
- Smoother skin texture
- Brighter complexion
- Faster removal of pigmented cells
Collagen Production
Retinoids stimulate fibroblasts to produce:
- Type I collagen
- Type III collagen
At the same time, they inhibit collagen-degrading enzymes.
This contributes to:
- Reduced wrinkles
- Improved elasticity
- Dermal remodeling
Anti-Inflammatory Activity
Retinoids suppress inflammatory pathways involved in acne and other skin disorders.
Pigment Regulation
Retinoids help disperse melanin and accelerate removal of pigmented keratinocytes.
This improves:
- Post-inflammatory hyperpigmentation
- Melasma
- Uneven skin tone
Importance of Retinoids in Modern Dermatology
Today, retinoids are considered indispensable in dermatologic practice.
Retinoids in Acne Management
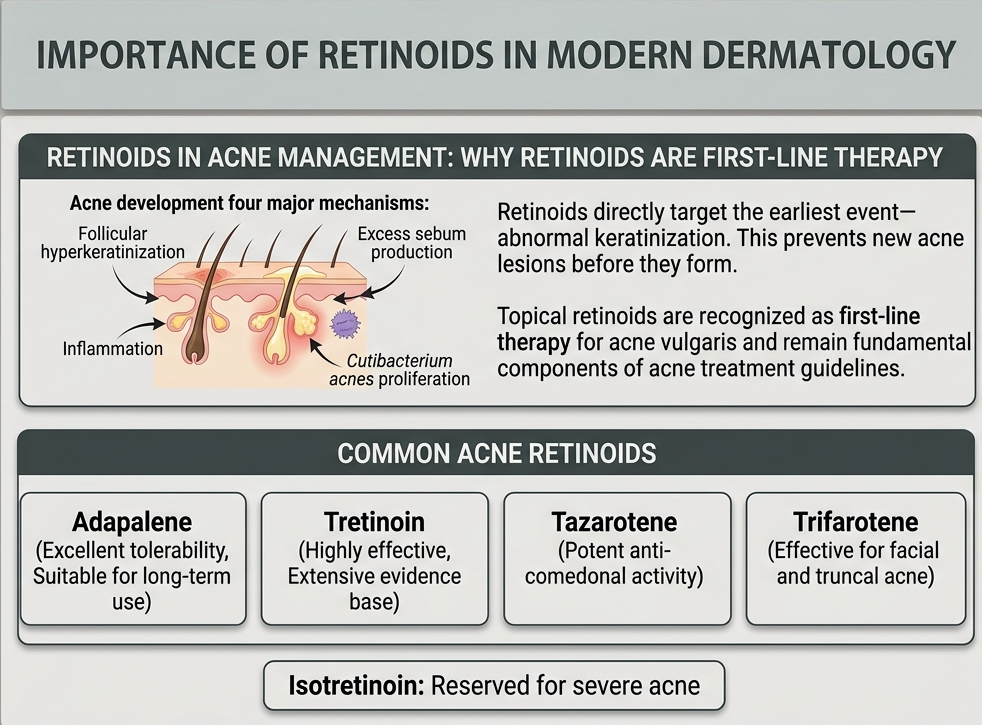
Why Retinoids Are First-Line Therapy
Acne develops through four major mechanisms:
- Follicular hyper keratinization
- Excess sebum production
- Inflammation
- Cutibacterium acnes proliferation
Retinoids directly target the earliest event-abnormal keratinization. This prevents new acne lesions before they form. Topical retinoids are recognized as first-line therapy for acne vulgaris and remain fundamental components of acne treatment guidelines.
Common Acne Retinoids
Adapalene
- Excellent tolerability
- Suitable for long-term use
Tretinoin
- Highly effective
- Extensive evidence base
Tazarotene
- Potent anti-comedonal activity
Trifarotene
- Effective for facial and truncal acne
Isotretinoin
- Reserved for severe acne
Retinoids in Photoaging

Understanding Photoaging
Photoaging results from chronic ultraviolet (UV) exposure.
Features include:
- Fine lines
- Wrinkles
- Pigmentation
- Loss of elasticity
- Rough texture
Why Retinoids Are the Gold Standard
Retinoids address the underlying biological changes associated with aging skin.
They:
- Stimulate collagen synthesis
- Reduce matrix metalloproteinases
- Increase epidermal thickness
- Improve dermal architecture
Tretinoin remains one of the most scientifically validated anti-aging treatments available. Multiple clinical studies demonstrate significant improvements in wrinkles, skin texture, and photoaged skin.
Clinical Benefits
Regular use may improve:
- Fine wrinkles
- Skin roughness
- Skin laxity
- Dullness
- Uneven texture
Retinoids in Pigmentation Disorders
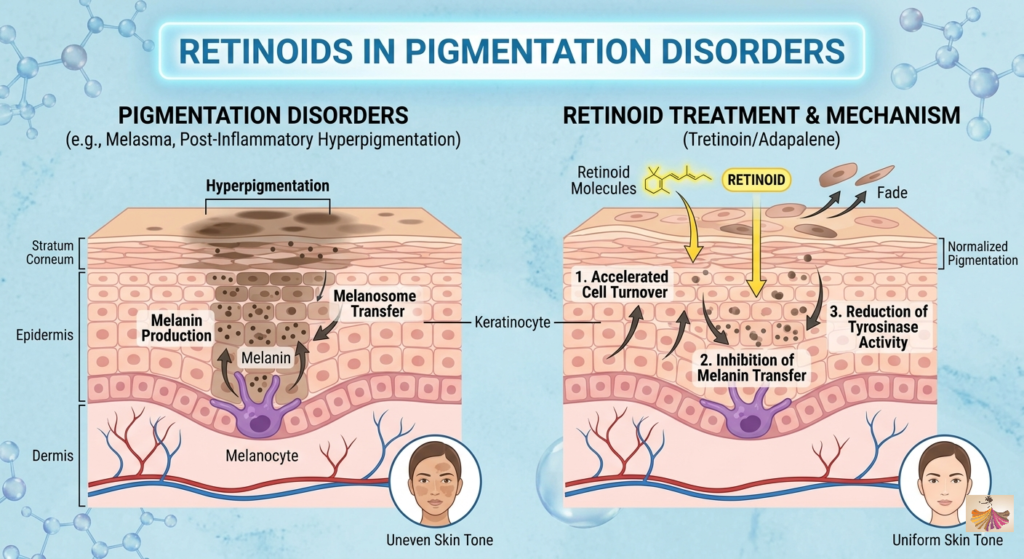
Hyperpigmentation
Hyperpigmentation results from excessive melanin accumulation.
Common causes include:
- Acne
- Sun exposure
- Hormonal changes
- Skin inflammation
Melasma
Melasma is a chronic pigmentary disorder characterized by brown facial patches.
Retinoids contribute by:
- Increasing epidermal turnover
- Enhancing penetration of depigmenting agents
- Reducing melanin transfer
Post-Inflammatory Hyperpigmentation
Retinoids are particularly useful for treating pigmentation following acne.
Benefits include:
- Faster pigment resolution
- Improved skin tone uniformity
- Prevention of recurrent acne lesions
Modern reviews identify retinoids as valuable therapeutic tools for pigmentary disorders, including melasma and post-inflammatory hyperpigmentation.
Emerging Trends in Retinoid Therapy
Recent advances focus on:
Receptor-Selective Retinoids
Designed to:
- Increase efficacy
- Reduce irritation
Examples include trifarotene.
Nanotechnology-Based Delivery Systems
Researchers are developing:
- Nanoemulsions
- Liposomes
- Solid lipid nanoparticles
These technologies may:
- Improve stability
- Enhance penetration
- Reduce adverse effects
Modern research suggests Nano-formulations may improve retinoid delivery and patient tolerability.
Combination Therapy
Current dermatology increasingly combines retinoids with:
- Benzoyl peroxide
- Antibiotics
- Azelaic acid
- Hydroquinone
- Chemical peels
- Laser therapies
This approach improves outcomes while minimizing resistance and recurrence.
Safety and Common Side Effects
Although highly effective, retinoids may cause:
- Dryness
- Peeling
- Erythema
- Burning sensation
- Photosensitivity
These effects are usually temporary and improve with continued use and proper moisturization.
Dermatologists often recommend:
- Gradual introduction
- Moisturizer support
- Daily sunscreen use
Conclusion
Retinoids represent one of the most important breakthroughs in dermatologic medicine. Derived from vitamin A, these compounds regulate gene expression, normalize epidermal differentiation, stimulate collagen production, reduce inflammation, and improve pigmentation. Their development from early vitamin A research to sophisticated receptor-selective molecules has transformed the treatment of acne, photoaging, hyperpigmentation, psoriasis, and numerous other skin disorders.
Today, retinoids remain the gold standard in acne therapy, the most evidence-based topical treatment for photoaging, and a critical component of management strategies for pigmentary disorders. With ongoing advances in receptor-selective agents, nanotechnology-based delivery systems, and combination therapies, the future of retinoid-based dermatology continues to expand.





