
Retinoid Therapy Explained: Comparing the Most Popular Vitamin A Derivatives
Introduction
Among all vitamin A derivatives used in dermatology, retinol, retinaldehyde (retinal), and tretinoin represent the most important members of the retinoid family. These compounds occupy different positions within the vitamin A metabolic pathway and exhibit distinct levels of potency, receptor activation, clinical efficacy, and tolerability.
The increasing popularity of anti-aging skincare, acne management, and pigmentation correction therapies has led to growing interest in understanding how these retinoids differ. While retinol dominates the over-the-counter (OTC) cosmetic market, retinaldehyde has emerged as an advanced next-generation OTC retinoid, and tretinoin remains the gold-standard prescription retinoid in clinical dermatology.
Understanding the biochemical conversion pathway from retinol to retinaldehyde and ultimately to retinoic acid is crucial because the number of metabolic steps directly influences efficacy, onset of action, and irritation potential. As dermatologic science advances, clinicians increasingly tailor retinoid selection according to patient goals, skin sensitivity, disease severity, and long-term treatment objectives.
Retinol
Definition
Alcohol Form of Vitamin A
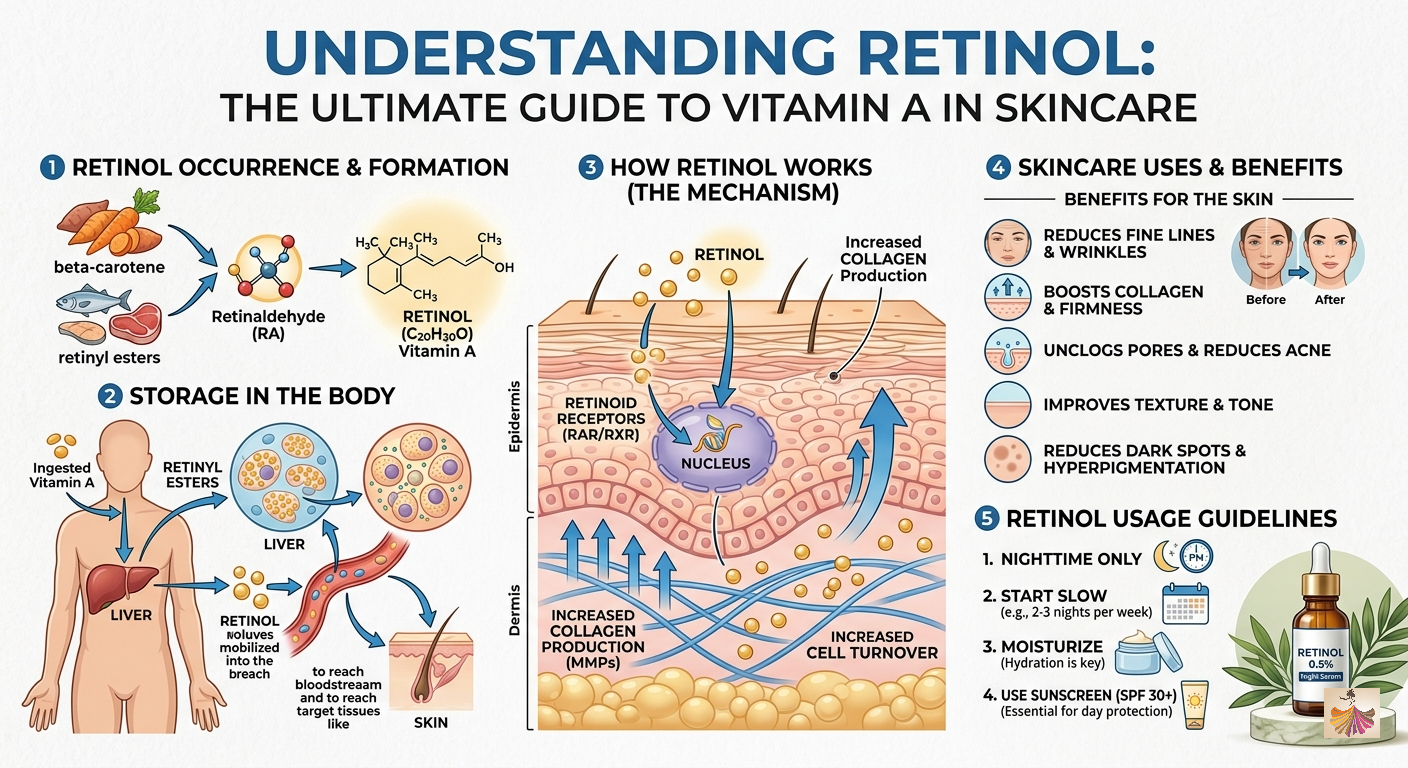
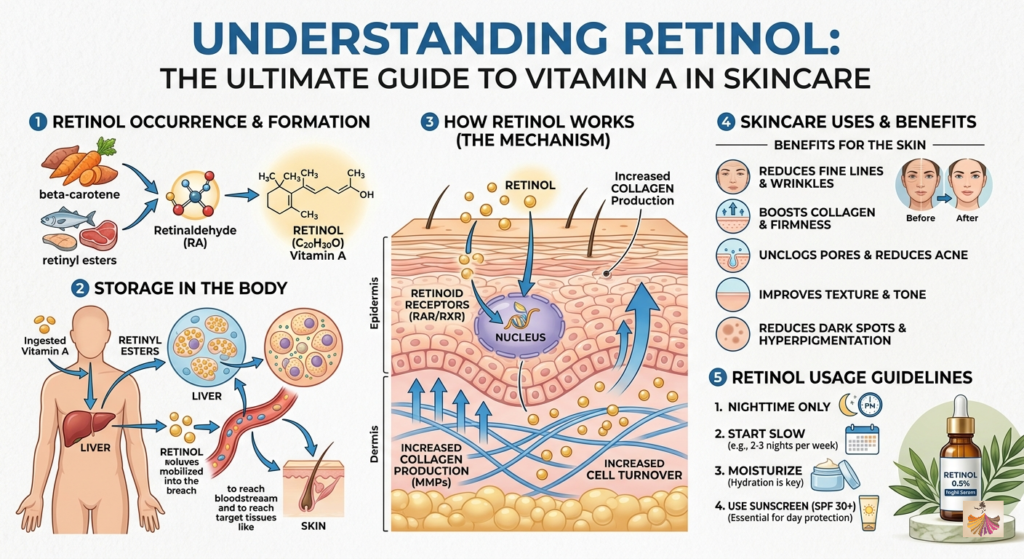
Retinol is the alcohol form of vitamin A and serves as one of the primary naturally occurring retinoids in human physiology. It is the most widely used non-prescription retinoid in cosmetic dermatology and skincare formulations. Retinol itself is not biologically active at the receptor level. Before exerting meaningful dermatologic effects, it must undergo enzymatic conversion within skin cells to produce retinoic acid, the active molecule that binds nuclear retinoid receptors. Because of its favorable balance between efficacy and tolerability, retinol remains one of the most extensively utilized ingredients in anti-aging skincare products worldwide.
Conversion Steps
Retinol → Retinal → Retinoic Acid
Retinol requires a two-step metabolic conversion process before becoming biologically active.
First Conversion
Retinol is oxidized into retinaldehyde (retinal) through the action of retinol dehydrogenase enzymes.
Second Conversion
Retinaldehyde is subsequently oxidized into retinoic acid by retinaldehyde dehydrogenases.
Only after completion of these two enzymatic reactions can the molecule activate retinoic acid receptors and regulate gene transcription. Because this conversion process is dependent on individual enzymatic activity, the clinical response to retinol varies significantly among patients.
Characteristics
Over-the-Counter Availability
One of retinol’s greatest advantages is its accessibility. Unlike prescription retinoids, retinol is widely available in cosmetic formulations without medical supervision. This OTC status has contributed to its popularity in preventive skincare and anti-aging routines.
Moderate Stability
Retinol exhibits greater stability than retinaldehyde and retinoic acid but remains susceptible to degradation when exposed to:
- Oxygen
- Light
- Heat
- Moisture
Modern formulations frequently utilize airless packaging, opaque containers, and stabilization technologies to preserve potency.
Lipophilic Molecule
Retinol is highly lipophilic, allowing efficient penetration through the lipid-rich stratum corneum. This characteristic enhances skin absorption and contributes to its usefulness in topical formulations.
Strength Profile
Lower Receptor Activation
Because retinol requires two enzymatic conversions before reaching its active form, only a fraction of the applied dose ultimately becomes retinoic acid. Consequently, retinol demonstrates lower receptor activation compared with retinaldehyde and tretinoin.
Slower Onset of Action
Clinical improvements generally appear after:
- 8–12 weeks for texture enhancement
- 12–24 weeks for pigmentation improvement
- Several months for visible anti-aging benefits
This delayed onset reflects the need for metabolic activation and gradual accumulation of biological effects. Contemporary reviews continue to show that retinol improves epidermal thickness, collagen synthesis, and skin texture but generally acts more slowly than prescription retinoids.
Clinical Uses
Mild Acne
Retinol can help normalize follicular keratinization and reduce microcomedone formation. Although less potent than prescription retinoids, it remains useful for:
- Mild acne
- Comedonal acne
- Acne maintenance therapy
Photoaging Prevention
Retinol is widely used to prevent and delay signs of skin aging.
Benefits include:
- Enhanced epidermal renewal
- Improved collagen production
- Reduced fine lines
- Better skin smoothness
Texture Improvement
Regular retinol use can improve:
- Skin roughness
- Uneven texture
- Dull complexion
- Early photodamage
These effects explain its widespread incorporation into preventive dermatologic skincare regimens.
Limitations
Variable Conversion Efficiency
One major limitation of retinol is that conversion to retinoic acid differs among individuals. Factors affecting conversion include:
- Age
- Genetic variation
- Skin condition
- Enzymatic activity
- Barrier integrity
Consequently, identical products may produce different outcomes in different users.
Formulation-Dependent Effectiveness
Retinol efficacy is heavily influenced by formulation science.
Important variables include:
- Encapsulation technology
- Vehicle composition
- Packaging
- Concentration
- Stabilization methods
Poorly formulated products may undergo significant degradation before reaching target tissues, reducing clinical effectiveness.
Retinaldehyde (Retinal)
Definition
Aldehyde Form of Vitamin A
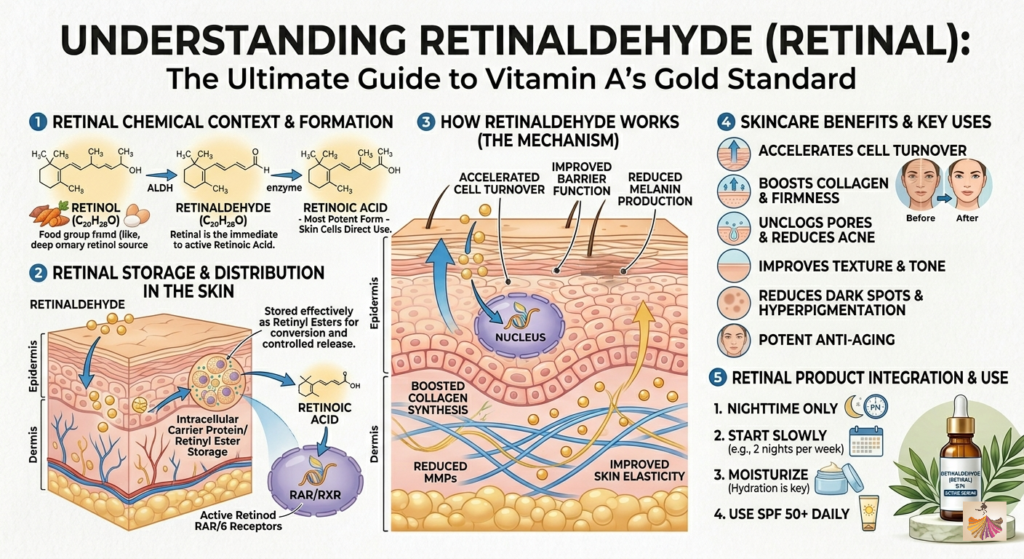
Retinaldehyde, commonly known as retinal, represents the aldehyde form of vitamin A. It occupies an intermediate position in the retinoid metabolic pathway between retinol and retinoic acid. In recent years, retinal has gained significant attention as a next-generation OTC retinoid due to its favorable balance between efficacy and tolerability.
Conversion Steps
Retinal → Retinoic Acid
Unlike retinol, retinal requires only a single enzymatic conversion step to become active.
Retinal is directly oxidized into retinoic acid by retinaldehyde dehydrogenase enzymes. This shorter metabolic pathway allows retinal to achieve higher biological activity and faster clinical results than retinol.
Characteristics
Intermediate Potency
Retinal occupies an intermediate position between retinol and tretinoin in terms of potency. This positioning provides an attractive option for patients seeking greater efficacy than retinol without the irritation frequently associated with tretinoin.
Higher Intrinsic Biological Activity
Because retinal is only one step away from retinoic acid, a larger proportion of the applied dose can be converted into the active form. Consequently, retinal often demonstrates greater biological activity at lower concentrations.
Increasing Use in Modern OTC Skincare
Recent years have witnessed rapid growth in retinal-containing formulations. Dermatologists increasingly recommend retinal for:
- Early photoaging
- Mild-to-moderate acne
- Pigmentation concerns
- Retinol non-responders
The rise of advanced encapsulation technologies has accelerated retinal’s popularity in modern skincare markets.
Mechanistic Advantages
Faster Conversion to Active Form
Retinal’s single-step conversion pathway enables faster production of retinoic acid within epidermal cells.
This results in:
- Earlier clinical improvement
- More efficient receptor activation
- Greater biological response
Higher Receptor Activation Efficiency
Compared with retinol, retinal generally achieves stronger downstream activation of retinoid signaling pathways because less metabolic processing is required. Studies have demonstrated enhanced epidermal remodeling, collagen stimulation, and anti-aging effects relative to comparable retinol formulations.
Clinical Uses
Acne Management
Retinal improves follicular differentiation and reduces microcomedone formation.
Benefits include:
- Reduced pore obstruction
- Decreased inflammatory lesions
- Improved skin turnover
Hyperpigmentation
Retinal supports pigment correction by accelerating epidermal renewal and promoting removal of melanin-containing keratinocytes. Clinical benefits include improvement of:
- Post-inflammatory hyperpigmentation
- Sun-induced pigmentation
- Uneven skin tone
Early Anti-Aging Intervention
Retinal has become increasingly popular among younger patients seeking proactive prevention of photoaging.
Benefits include:
- Improved collagen synthesis
- Enhanced skin elasticity
- Reduction of fine lines
- Improved luminosity
Formulation Considerations
Stability Challenges
Despite its advantages, retinal is chemically unstable.
Major threats include:
- Oxidation
- Light exposure
- Temperature fluctuations
These challenges complicate manufacturing and storage.
Encapsulation and Liposomal Delivery Systems
To overcome instability, manufacturers increasingly utilize:
- Liposomes
- Nanoencapsulation
- Polymeric delivery systems
- Controlled-release formulations
Such technologies improve retinal stability while enhancing skin penetration and reducing irritation.
Controversies in Literature
Variable Evidence Regarding Superior Tolerability
Although retinal is frequently marketed as less irritating than retinol, scientific evidence remains mixed. Several studies support improved efficacy with acceptable tolerability, whereas other analyses suggest that observed differences may be largely attributable to formulation design rather than the molecule itself.
Strong Dependence on Formulation Technology
A growing body of literature emphasizes that retinal’s clinical performance depends heavily on stabilization and delivery systems. Experts increasingly recognize that formulation quality may influence outcomes as much as the retinal molecule itself. Modern reviews therefore recommend evaluating both retinal concentration and formulation technology when assessing product efficacy.
Tretinoin (All-Trans Retinoic Acid)
Definition
Active Carboxylic Acid Form of Vitamin A
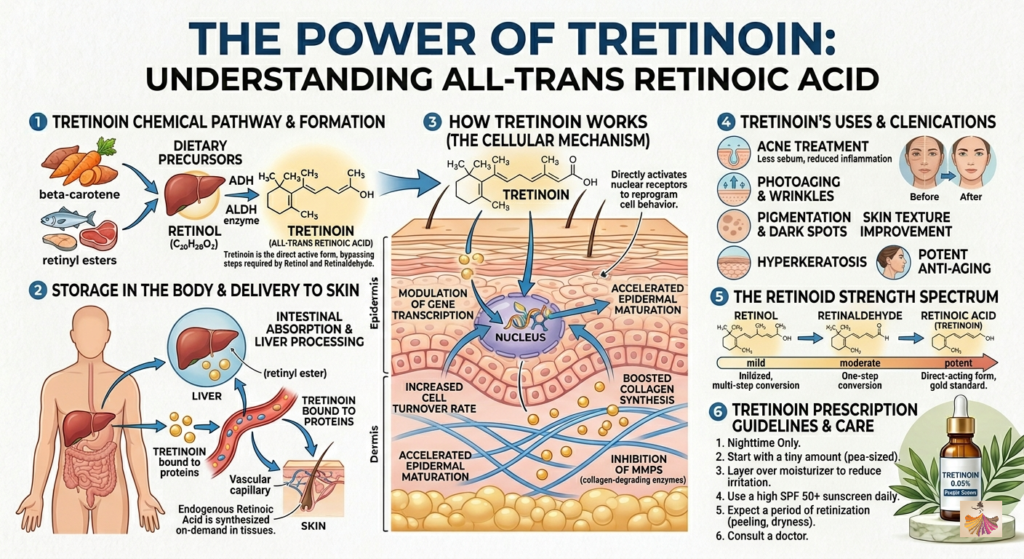
Tretinoin, also known as all-trans retinoic acid, is the biologically active carboxylic acid derivative of vitamin A. Unlike retinol and retinaldehyde, tretinoin does not require metabolic activation before exerting biological effects. It remains the most extensively studied topical retinoid in dermatology and serves as the benchmark against which other topical retinoids are compared.
Conversion Steps
No Conversion Required
Tretinoin is already in its active form. After topical application, it directly binds retinoic acid receptors within target cells. This direct activity explains its superior potency and faster clinical response.
Characteristics
Prescription-Only Topical Drug
In most countries, tretinoin is regulated as a prescription medication due to its pharmacologic potency and potential adverse effects. Common concentrations include:
- 0.025%
- 0.05%
- 0.1%
Available formulations include:
- Creams
- Gels
- Microsphere formulations
- Lotion systems
Highest Receptor Binding Activity
Tretinoin directly activates retinoic acid receptors without requiring enzymatic conversion. This results in stronger and more predictable biologic effects than precursor retinoids.
Mechanism Intensity
Direct RAR Activation
Tretinoin binds directly to:
- RAR-α
- RAR-β
- RAR-γ
Activation of these receptors regulates numerous genes involved in epidermal proliferation, differentiation, inflammation, collagen production, and pigmentation.
Strong Gene Transcription Modulation
Tretinoin influences expression of hundreds of genes involved in skin physiology. Consequences include:
- Increased epidermal turnover
- Enhanced collagen synthesis
- Reduced matrix metalloproteinases
- Improved keratinocyte differentiation
- Modulation of inflammatory pathways
These powerful genomic effects explain its unparalleled clinical efficacy.
Clinical Uses
Acne Vulgaris (Gold Standard)
Tretinoin remains the gold-standard topical retinoid for acne management.
Benefits include:
- Prevention of microcomedones
- Reduction of inflammatory lesions
- Improved follicular turnover
- Long-term acne control
Recent dermatology reviews continue to identify tretinoin as one of the most effective topical therapies for acne vulgaris.
Photoaging Reversal
Tretinoin is considered the gold-standard topical treatment for photoaged skin.
Clinical studies demonstrate improvements in:
- Fine wrinkles
- Skin roughness
- Dyspigmentation
- Dermal collagen content
A 2024 systematic review reaffirmed tretinoin’s position as the benchmark anti-aging therapy in dermatology.
Melasma and Hyperpigmentation
Tretinoin promotes melanin dispersion and accelerates epidermal turnover.
Consequently, it is commonly incorporated into treatment regimens for:
- Melasma
- Post-inflammatory hyperpigmentation
- Photodamage-associated pigmentation
Keratinization Disorders
Tretinoin is also valuable in disorders characterized by abnormal keratinocyte differentiation, including several hyperkeratotic and keratinization-related dermatoses.
Therapeutic Profile
Fastest Onset of Visible Clinical Effect
Because tretinoin is already biologically active, it generally produces clinical improvements faster than retinol and retinal.
Patients often observe:
- Acne improvement within 6–12 weeks
- Texture enhancement within several weeks
- Progressive anti-aging benefits over months
Highest Irritation Potential
The major limitation of tretinoin is irritation.
Common adverse effects include:
- Erythema
- Peeling
- Dryness
- Burning
- Increased photosensitivity
The initial retinization period may last several weeks. Despite these limitations, the superior efficacy of tretinoin continues to make it the preferred choice for patients requiring maximum therapeutic benefit. Modern systematic reviews consistently conclude that while alternative retinoids may offer better tolerability, tretinoin remains the reference standard for efficacy.
Conclusion
Retinol, retinaldehyde, and tretinoin represent a progressive spectrum of retinoid potency. Retinol offers accessibility and excellent tolerability but requires two conversion steps before becoming active. Retinaldehyde provides enhanced biological activity through a single conversion step and is increasingly recognized as a powerful OTC option. Tretinoin, the active form of retinoic acid, delivers the strongest receptor activation, fastest clinical response, and most robust evidence base for acne, photoaging, pigmentation disorders, and keratinization abnormalities.
As modern dermatology continues to evolve, individualized retinoid selection based on patient needs, skin sensitivity, treatment goals, and formulation science remains central to achieving optimal clinical outcomes. The growing emphasis on advanced delivery systems and receptor-targeted therapies is expected to further refine retinoid treatment strategies in the coming years.





